HFpEF with CKD with HTN
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
60 y/o female came to the casuality with the chief complaints of
1. SOB since the past 8 days
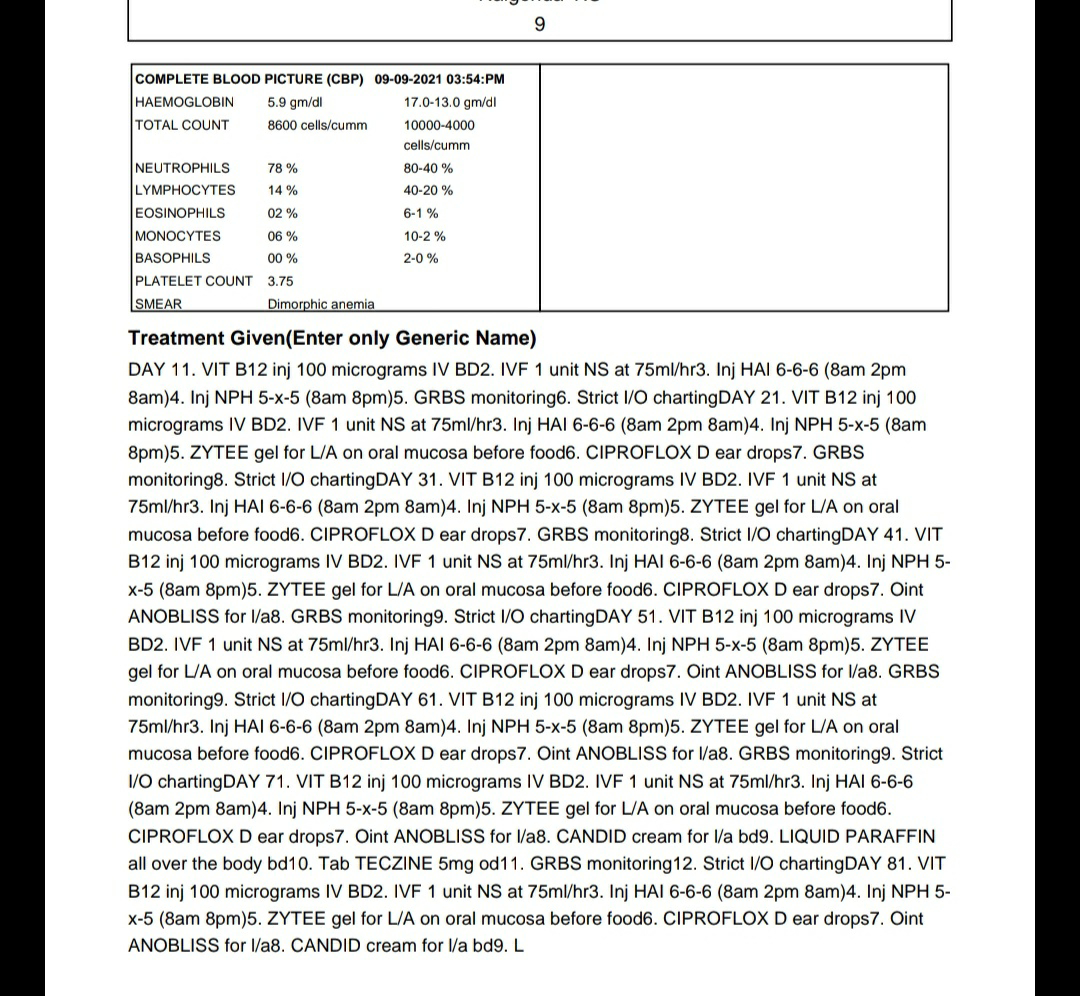
The patient was apparantly asymptomatic 8 days ago. At 2pm she developed an episode of SOB. Orthopnoea + and PND +. It lasted for 2 hours. She was taken to local RMP. SOB resolved on medication. The next day patient was take to a private hospital at Suryapet. There diagnosis of anemia (Hb 3.4, RBC 1.1 million, PCV 10.2, TLC 9500) was made and blood transfusion was adviced which the patient refused.
2 years back, she developed pedal edema (pitting type, upto knee) not a/w facial puffiness, reduced urine output. The patient was taken to nearby doctor and was diagnosed to have renal failure l. Tab DYTOR 5mg and Tab NODOSIS 50mg po/bd for 5 days. She was not followed up further.
K/C/O HTN since 4 years (on Tab AMLONG 5mg po/od)
Not a K/C/O DM, TB, asthma, epilepsy.
The patient is married. Currently unemployed and stays at home. She used to be a farmer.
Now she has reduced appatite
Takes vegetarian diet
Bowels irregular
Micturition normal
No known allergies
No addictions
On Examination
Pt is C/C/C
Thin built and undernourished
Pallor severe
No icterus, cyanosis, lymphadenopathy, clubbing, pedal edema
Dehydrated - mild
Afebrile
PR 86bpm
BP 100/60 mmHg
RR 24 cpm
SpO2 100% at room air
CVS
S1 S2 heard
JVP elevated
RS
Dyspnoea +
Wheeze -
Trachea central
Breath sounds vesicular
P/A
Soft, non-tender, bowel sounds +
CNS
Pt is conscious
Speech normal
No signs of neck stiffness
Cranial nerves, motor and sensory system normal
GCS 15/15
Reflexes R L
1. Biceps 2+ 2+
2. Triceps + +
3. Supinator - -
4. Knee + +
5. Ankle + +
Prov Diagnosis
HFpEF with CKD with HTN
High risk consent taken
Consent for central line insertion taken
Central line insertion
1. Indication - Hemodialysis
2. Site - R IJV
3. Technique - Mod. Seldinger Technique
Post procedure x ray taken
Hemodialysis performed at 1:30 am with 1 unit PRBC transfusion for uremic encephalopathy (elevated blood urea and creatinine).





SOAP NOTES DAY 0
ICU 6TH BED
S
Pt is C/C/C
Has SOB
Pedal edema
O
Pallor +
Icterus -
Cyanosis -
Clubbing -
Lymphadenopathy -
Pedal edema -
Afebrile
BP 100/60 mmHg
PR 86 bpm
RR 24 cpm
SpO2 100 at room air
A
HFpEF with CKD with HTN with severe anemia
P
1. Fluid restriction < 1.5 L
2. Salt restriction < 2gm
3. Inj LASIX 40mg iv/od
4. Inj ONDONSETRON 4mg iv/sos
5. Tab NICARDIA 20mg po/od
6. Inj PANTOP 40mg iv/od
7. Tab OROFER XT po/bd
8. Tab NODOSIS 550mg po/bd
9. BP PR RR Temp 4th hrly monitoring
10. I/O charting
11. Tab SHELCAL 500mg po/bd
12. Inj AUGMENTIN 1.2g iv/bd
SOAP NOTES DAY 1
ICU 6TH BED
S
Pt drowsy
Tachypnoeic
GCS E2V3M4
O
Pallor +
Icterus -
Cyanosis -
Clubbing -
Lymphadenopathy -
Pedal edema -
Afebrile
BP 150/80 mmHg
PR 115 bpm
RR 20 cpm
I/O 100/200
Stools not passed
GRBS 120mg/dl
A
CKD with Anemia secondary to ? CKD with HFpEF with HTN with ?ARDS
P
1. Head end elevation
2. BIPAP Intermittently 2nd hrly with O2 to maintain sats above 94%
3. Inj LASIX 40mg iv/bd (8am 4pm), if SBP more than 110 mmHg
4. Inj PANTOP 40mg iv/od
5. Inj ZOFER 4mg iv/sos
6. Inj AUGMENTIN 1.2gm iv/bd (D3)
7. Tab NICARDIA 20mg po/bd
8. Tab OROFER XR po/bd
9. Tab NODOSIS 550mg po/bd
19. Tab SHELCAL 500mg po/bd
11. Vitals monitoring 4th hrly
12. I/O charting
SOAP NOTES DAY 2
ICU 6TH BED
S
Pt altered sensorium
Drowsy
SOB +
GCS E2V3M3
Saturation dropping to 75
I/O 200/350
Stools not passed
O
Pallor +
Clubbing -
Icterus +
Pedal edema -
Afebrile
PR 102 BPM
BP 160/90 mmHg
RR 25
GRBS 122mg/dl
CVS S1 S2 +
RS B/L coarse crepts
P/A soft, non-tender
CNS E2V3M3
RFT
Urea 57
Creat 3
UA 2.9
Ca 9.4
P 4.4
Na 140
K 3.7
Cl 96
ABG
pH 7.37
pO2 48.3
pCO2 30.1
HCO3 C 17.2
HCO3 ST 18.8
A
CKD with Anemia secondary to ?CKD with HFpEF with HTN with ?ARDS/?Cardiogenic Pul Edema
P
1. Ryle's tube feed (200ml milk 4th hrly, 100ml water hrly)
2. Head end elevation
3. BIPAP Intermittently 2nd hrly with O2 to maintain sats above 94%
4. Inj LASIX 40mg iv/bd (8am 4pm)
5. Inj PANTOP 40mg iv/od
6. Inj ZOFER 4mg iv/sos
7. Inj AUGMENTIN 1.2gm iv/bd (D3)
8. Tab NICARDIA 20mg po/bd
9. Tab OROFER XR po/bd
10. Tab NODOSIS 550mg po/bd
11. Tab SHELCAL 500mg po/bd
12. Vitals monitoring 4th hrly
13. I/O charting

SOAP NOTES DAY 3
ICU 6TH BED
S
Pt altered sensorium
Drowsy but arousable
SOB +
GCS E3V1M1
Saturation 92 at 16L O2
I/O 1500/900
Stools not passed
O
Pallor +
Clubbing -
Icterus +
Pedal edema -
Pupils pin point, equal on both sides. Non reactive to light
Afebrile
PR 70 BPM
BP 130/70 mmHg
RR 22
GRBS 219 mg/dl
CVS S1 S2 +
RS B/L inspiratory crepts at IAA, IMA, ISA
P/A soft, non-tender
Reflexes
Reflexes R L
1. Biceps + +
2. Triceps - -
3. Supinator - -
4. Knee + +
5. Ankle + +
6. Plantar mute mute
ABG
pH - 7.111
pCO2 - 72.2
pO2 - 11p
HCO3 c - 22.0
HCO3 st - 18.6
Urea
Creat
Na
K
Cl
A
CKD with Anemia secondary to ?CKD with HFpEF with HTN with ?ARDS/? Non-Cardiogenic Pul Edema
P
1. Ryle's tube feed (200ml milk 2nd hrly with protein powder, 100ml water hrly)
2. Head end elevation
3. O2 inhalation to maintain O2 sat at above 94%
4. BIPAP Intermittently 2nd hrly
5. Inj LASIX 40mg iv/bd (8am 4pm)
6. Inj PANTOP 40mg iv/od
7. Inj ZOFER 4mg iv/sos
8. Inj AUGMENTIN 1.2gm iv/bd (D3)
9. Tab AMLONG 5mg po/od
10. Tab NODOSIS 550mg po/tid
11. Nebulisation with BUDECORT 12th hrly, IPRAVENT 6th hrly
12. Vitals monitoring 4th hrly
13. I/O charting