Vestibular Neuronitis
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
45 year old lady presented with the complaints of
1. Vomiting (4 episodes) since yesterday morning
2. Giddiness since 4 hrs
The patient was apparantly asymptomatic till yesterday morning. Then she developed vomitings. The
vomitings vere non-projectile, non-bilious, content was food particles and non-foul smelling. She had
some coconut water after 2 hours. She vomited it after 10 minutes. Then she went to the local RMP
and had another 2 episodes of vomitings.From 4 hours, the patient has giddiness.
No complaints of fever, headache, lose stools, pain abdomen, pedal edema, chest pain and
palpitations.
Past History
Not a known case of DM, HTN, TB, asthma or epilepsy.
Personal history
Diet - mixed
Appatite - reduced
Sleep - adequate
Bowel and bladder movements - regular
Addictions - none
General Examination
The patient was
C/C/C
Afebrile
Moderately built and nourished
No pallor, icterus, cyanosis, clubbing, lymphadenopathy
BP 140/80mmHg
PR 62 BPM
GRBS 141mg/dl
SpO2 98%
CVS S1 S2 heard
RS BAE+
P/A soft, non tender
CNS - No FAD
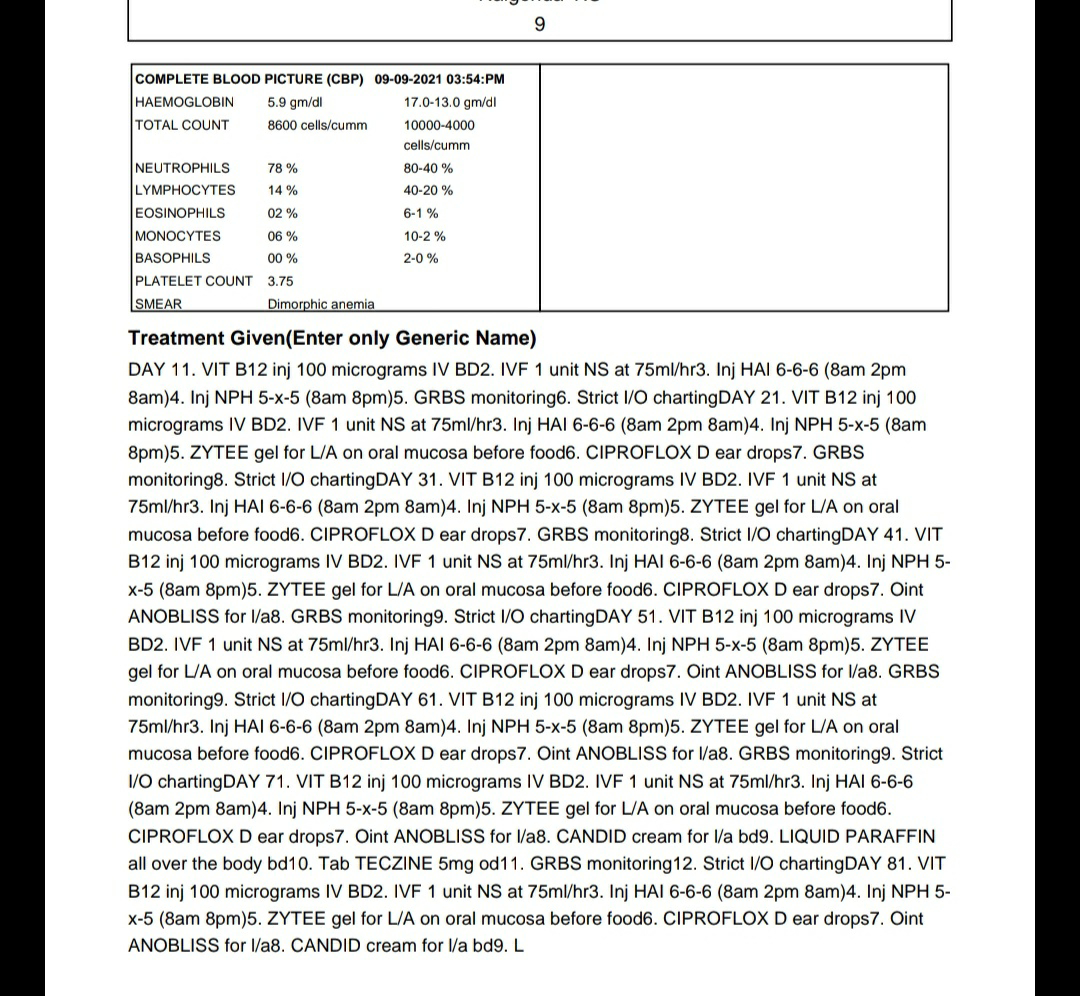
INVESTIGATIONS
1.Hemogram











COURSE IN THE HOSPITAL
Day 0
SOAP Notes
Subjective
C/o vomitings (4 episodes) and giddiness
Objective
Pallor +
Clubbing -
PR - 89 bpm
BP - 120/80mmhg
Afebrile
Spo2 - at 99% on RA
RR - 19 cpm
CVS - S1 S2 +
RS - BAE +
CNS - No FAD
Per Abdomen - Soft, non-tender, Bowel sounds +
AssessmentGastritis
Plan of treatment
1. Inj PAN 80mg in 500ml NS at 100ml/hr
2. Inj ZOFER 4 mg IV TID
3. IVF 1NS, 1RL at 75ml/hr
4. GRBS Charting 6th hourly
5. BP, PR, RR, Temp, SpO2 monitoring 4th hourly
Day 1
Patient taken for ENT referral for giddiness. Xray C spine AP and lateral were taken. The following
treatment was advised
1. Tab VERTIN 16mg for 5 days
2. DEE WAX Ear drops for 5 days




SOAP Notes
Subjective
C/o vomitings (4 episodes) and giddiness
Objective
Pallor +
Clubbing -
PR - 81 bpm
BP - 110/80mmhg
Afebrile
Spo2 - at 99% on RA
RR - 16 cpm
CVS - S1 S2 +
RS - BAE +
CNS - No FAD
Per Abdomen - Soft, non-tender, Bowel sounds +
AssessmentGastritis
Plan of treatment
1. Inj PAN 40mg IV OD
2. Inj ZOFER 4 mg IV TID
3. Tab PROMETHAZINE 25mg PO BD
4. IVF 1NS, 1RL at 75ml/hr
5. GRBS Charting 6th hourly
6. BP, PR, RR, Temp, SpO2 monitoring 4th hourly
Provisional Diagnosis
VESTIBULAR NEURONITIS
? GASTRITIS