? FEVER UNDER EVALUATIONUNCONTROLLED SUGARS (DENOVO DM)K/C/O HTN SINCE 5 YEARS
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 65 year old female , who was agricultural labourer came to the casuality with chief complaints of
- FEVER since 4 days
- SHORTNESS OF BREATH since 4 days
HISTORY OF PRESENT ILLNESS:
Patient was apparently asymptomatic 4 days back then she developed fever which was high grade associated with chills and rigor,present through out the day , with no diurnal variation and fever relieved on taking medications.
Fever was not associated with rash, nausea, vomiting, malena and pain abdomen
C/o shortness of breath (initially grade 2 and then gradually progressed to grade 3) according to NYHA classification.
For the above complaints she was taken to a nearby RMP and was diagnosed with Denovo-DM and was put on medication (Voglife-GM1) and was referred to KIMS
PAST HISTORY:
She was a k/c/o HTN since 5 years and was on regular medication (TELMIKIND 40)
Not a k/c/o TB,Asthama, CAD/CVA ,Thyroid and epilepsy
She underwent tubectomy 23 years back
PERSONAL HISTORY:
Mixed diet
Sleep adequate
Appetite - normal
Bowel and bladder movements regular
No addictions
GENERAL EXAMINATION :
- Patient is conscious, coherent, co-operative.
Moderately built and moderately nourished
- No pallor, cyanosis, clubbing,icterus koilonychia, lymphadenopathy and edema
VITALS:
Temperature- Afebrile
Pulse rate- 86 bpm
Respiratory Rate- 24 cpm
BP-150/100 mmHg
SPO2 at room air- 98%
GRBS 405 mg/dl
SYSTEMIC EXAMINATION:
CVS
S1, S2 heard , No murmurs
RS :
Position of trachea: central
Bilateral air entry +
Normal vesicular breath sounds - heard
No added sounds.
PER ABDOMEN:
Abdomen is soft and non tender.
No organomegaly.
Bowel sounds heard.
CNS:
Patient is Conscious
Speech: normal
No signs of Meningeal irritation
Motor & sensory system: normal
Reflexes: present
Cranial nerves: intact
PROVISIONAL DIAGNOSIS:
? DIABETIC KETOACIDOSIS
INVESTIGATIONS
On day 15/08/2021
CXR

ECG

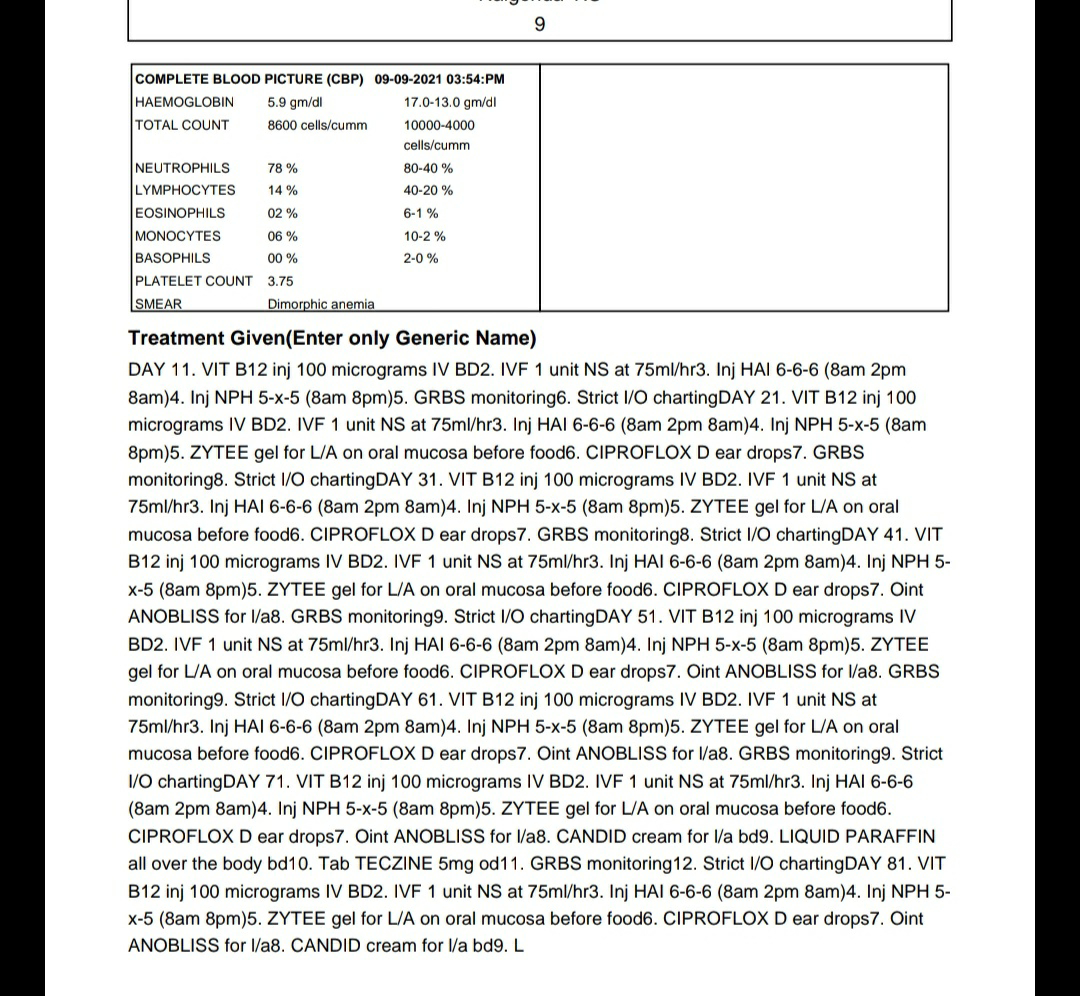
HEMOGRAM

CUE

URINE FOR KETONE BODIES
Negative

ABG

SERUM ELECTROLYTES

SERUM CREATININE
0.9 mg/dl

BLOOD UREA
40 mg/dl

LFT

HBA1C
7.6 %

RBS
459 mg/dl

DENGUE NS1 ANTIGEN
Negative

BLOOD PARASITES (M.P)
Negative

HIV 1/2 RAPID TEST
Non reactive

USG ABDOMEN

PROVISIONAL DIAGNOSIS
? FEVER UNDER EVALUATION
UNCONTROLLED SUGARS (DENOVO DM)
K/C/O HTN SINCE 5 YEARS
TREATMENT :
Day 1
1. IV Fluids (NS) 100ml/hr
2. Inj. HAI infusion acc to algorithm 1
3. Inj Pantop 40mg iv od
4. GRBS charting hourly
5. I/O charting
6. Tab DOLO 650mg/PO/TID
7. Inj NEOMAL 100ml/IV
8. Inj MONOCEF 1gm/IV/BD